Structural features and advantages
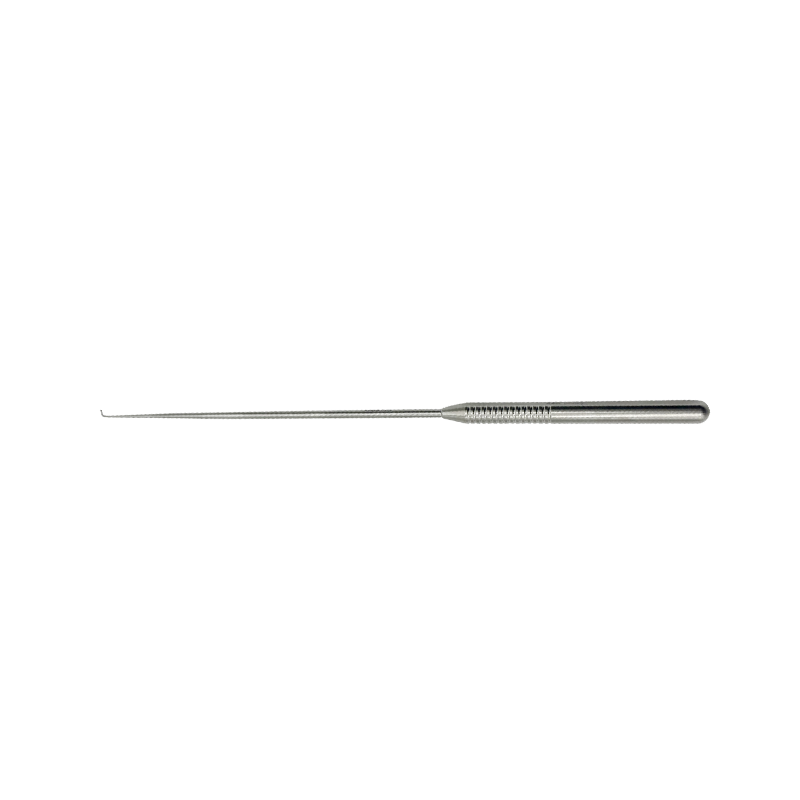
Size advantage
The 2MM diameter makes the nerve retractor have excellent passability in UBE surgery. In spinal surgery, the surgical channel is relatively narrow, especially in the cervical and thoracic areas. The smaller size allows the nerve retractor to enter the surgical site smoothly without causing excessive compression on the surrounding tissue. This helps to approach the nerve structure in a limited space, such as flexibly reaching around the nerve when operating in delicate areas such as the cervical intervertebral foramen or thoracic spinal canal.
Ball head design advantage
Reducing the risk of nerve injury: The ball head design is a key feature of the nerve retractor. The ball head has a smooth surface and no sharp edges, which can minimize the risk of cutting or contusion of the nerve when separating and pulling the nerve tissue. In spinal surgery, the nerve tissue is very fragile, such as the spinal cord and nerve roots. This design can safely separate the nerve from the surrounding tissue and avoid iatrogenic nerve injury caused by the instrument.
Good tissue adaptability: The ball head can better fit the surface of the nerve and the irregular shape of the surrounding tissue. When dealing with adhesion tissue around nerves or finding nerve paths in complex anatomical structures, the ball head can be operated along the contour of the nerve, improving the accuracy and efficiency of separation. For example, in lumbar disc herniation surgery, the ball head of the nerve retractor can follow the direction of the nerve root and gently separate it from the protruding disc tissue.
Application scenarios in UBE surgery
Application in disc herniation surgery
In UBE surgery for lumbar disc herniation or cervical disc herniation, the nerve retractor is used to protect and retract the nerve root. After endoscopically locating the protruding nucleus pulposus and compressed nerve root, the 2MM ball-headed nerve retractor can be gently inserted between the nerve and the nucleus pulposus from the side or below. The ball head can fit the shape of the nerve root and slowly retract it, allowing the doctor to see the protruding nucleus pulposus more clearly while avoiding damage to the nerve root. For example, in common intervertebral disc herniation segments such as L4-L5 or C5-C6, the nerve retractor creates good operating conditions for nucleus pulposus removal surgery while ensuring the safety of the nerve roots, effectively relieving the patient's nerve compression symptoms in the lower or upper limbs.
Application of spinal canal decompression surgery
In UBE surgery for spinal stenosis, the nerve retractor can be used to separate the nerve tissue in the spinal canal from the surrounding compressive tissue, such as the yellow ligament and bone hyperplasia. In cervical or lumbar spinal canal decompression surgery, when dealing with the hypertrophic yellow ligament on the posterior wall of the spinal canal, the nerve retractor can gently pull away the spinal cord or nerve roots located below the yellow ligament to prevent damage to the nerve during the removal of the yellow ligament. For lateral recess stenosis caused by bone hyperplasia on the lateral wall of the spinal canal, the nerve retractor can also help separate the nerve from the bone, providing safety for subsequent bone removal operations.
Application of spinal trauma surgery
In traumatic surgeries such as spinal fractures and dislocations, the nerve retractor can be used to inspect and protect nerve tissue. For example, in surgeries with thoracic vertebral fractures and the risk of spinal cord injury, nerve retractors can carefully explore the situation around the spinal cord before fracture reduction and fixation, separate the bone fragments or hematoma tissue that may compress the spinal cord from the spinal cord, and use retractors to gently pull the spinal cord apart to ensure the safety of the spinal cord during fracture reduction.
Operation precautions and skills
Operation precautions
Visual operation is crucial: UBE surgery relies on endoscopic visualization. Before using the nerve retractor, it is necessary to ensure that the endoscopic field of view is clear and accurately judge the relationship between the retractor and surrounding tissues such as nerves and blood vessels. Any blind operation may lead to serious consequences such as nerve damage.
Gentle operation principle: Due to the fragility of nerve tissue, the principle of gentleness must be followed during the operation. When inserting and pulling the nerve retractor, avoid excessive force to prevent pulling damage to the nerve. Especially when the nerve is already in a compressed or damaged state, it is necessary to operate more carefully.
Pay attention to the position of the retractor: During the operation, pay attention to keeping the position of the nerve retractor stable to avoid accidental movement during the surgical operation (such as tissue removal, flushing, etc.) and damage to the nerve. If the position of the retractor needs to be adjusted, it should be done slowly under direct vision.
Operation skills
Insertion skills: According to the anatomical path and nerve position observed by the endoscope, slowly insert the nerve retractor at an appropriate angle and direction. During the insertion process, use its 2MM diameter to carefully enter the area around the nerve along the natural anatomical gap or the established working channel to avoid forced insertion and damage to the surrounding tissue. For example, in anterior cervical spine surgery, when inserting the nerve retractor, you can first insert it along the gap at the front edge of the vertebral body, and then slowly adjust the direction to approach the nerve root.
Traction skills: When pulling the nerve, use gentle and continuous force. First, fully contact the ball head with the surface of the nerve, and then gradually apply tension to gradually separate the nerve from the surrounding tissue. The direction of traction should be determined according to the anatomical direction of the nerve and the needs of the surgical operation. Generally, the nerve is pulled along the natural extension direction to avoid twisting or over-bending the nerve. At the same time, combined with real-time observation of the endoscope, the strength and angle of traction should be flexibly adjusted according to the reaction of the nerve and the changes in the surrounding tissue.
 English
English عربى
عربى Español
Español